It is difficult to compare these techniques, they are not equivalent.
PRP treatment triggers skin rejuvenation from the inside with the body's own resources.
Mesotherapy is a skin strengthening treatment with mesococktails containing large amounts of nutrients.
Mesotherapy and PRP treatment are popular techniques in aesthetics. Both technologies can be used to correct signs of aging, improve skin tone, restore balance and activate natural rejuvenation processes. However, PRP and mesotherapy have significant differences, knowledge of which will allow you to choose the appropriate method.
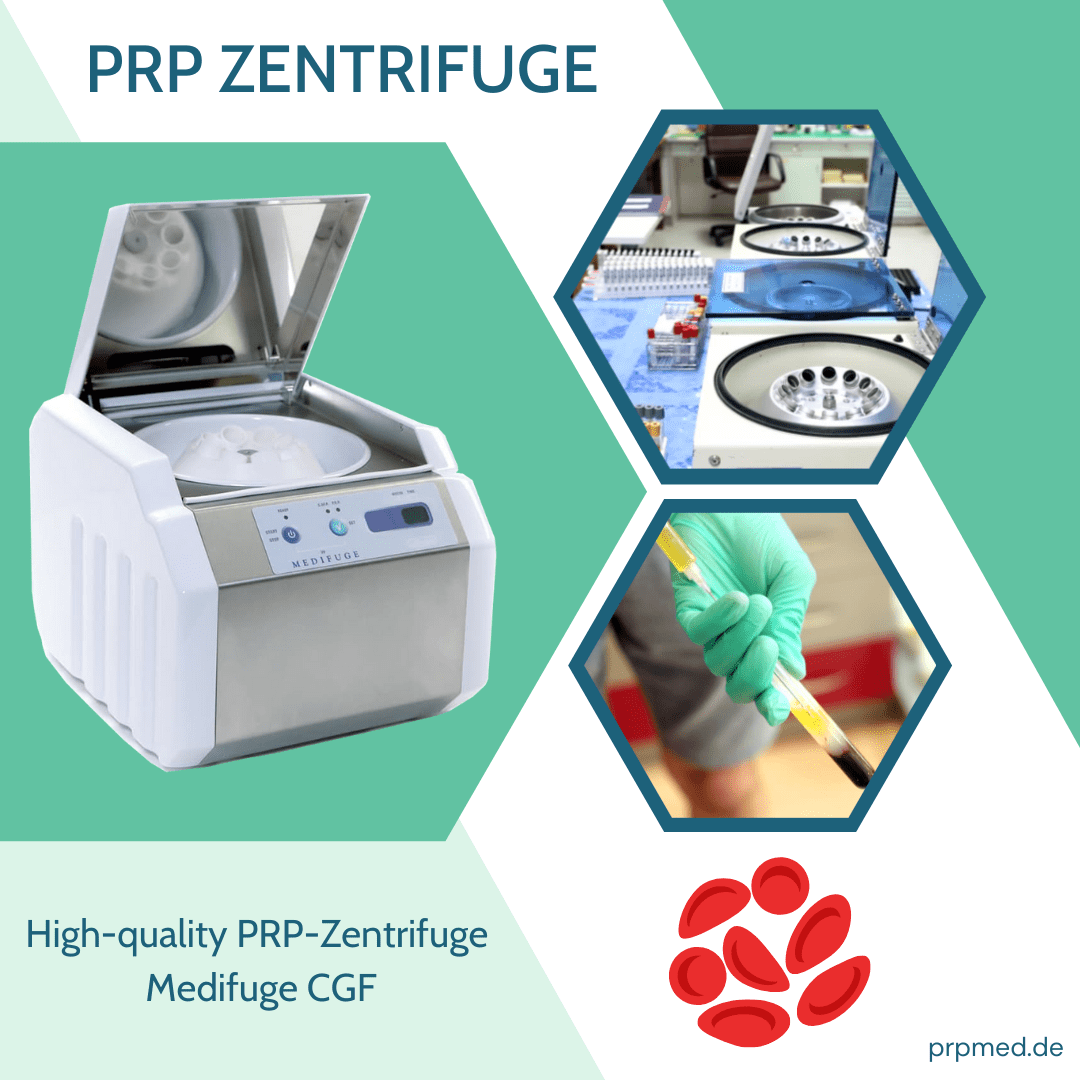
Both technologies are an injection of active substances into the skin layer of the face and décolleté. For the PRP method, plasma from the patient's own blood is used. For this purpose, the required amount of blood is taken from a vein and centrifuged to separate the red blood cells. The obtained plasma is rich in vitamins and amino acids, which are necessary to eliminate the signs of aging.
In mesotherapy, the role of plasma is taken over by a cocktail of vitamins with an enriched composition. The solutions may contain hyaluronic acid, vitamins B and C, acids, collagen and elastin.
PRP is used not only on the face, but also for the décolleté area and for scalp treatment.
Indications for PRP are:
" Elimination of hair loss, normalization of sebaceous glands on the head, elimination of dandruff and fungus;
" Treatment of acne;
" Minimization of wrinkles on the face and décolleté;
" Elimination of stretch marks and scars;
" Restoration of the water balance of the skin.
Mesotherapy is not designed to effectively eliminate baldness and address pronounced scalp problems, but it offers more ways to work with the body.
Indications for mesotherapy:
" Elimination of cellulite, stretch marks;
" Minimization of wrinkles;
" Elimination of pigmentation;
" Restoration of the water balance of the skin, normalization of skin color;
" Improvement of the natural turgor of the skin.
Both technologies have a common list of contraindications. Contraindications include herpetic inflammation, recent peeling, hemophilia, pregnancy and lactation.
Principles of treatment
PRP treatment requires a lengthy preparation period. Before the procedure, the patient is prescribed general and biochemical blood tests, as well as tests for infections (HIV, syphilis, hepatitis). If the test results are good, the procedure can be performed.
Mesotherapy treatment does not require extensive preparation, as a special vitamin cocktail is used for the injections.
Side effects
Both techniques have a number of side effects, which are the formation of small bruises at the injection sites. In PRP, the possibility of allergies is eliminated because the skin layer is injected with the body's own cells. In mesotherapy, cocktails of components of synthetic and plant origin are used, so there is a possibility of allergies. Before a session, the doctor must consider these points to rule out allergic reactions.
To choose the best technology for your rejuvenation, we recommend that you see a doctor who will help you make the right decision after an examination. We also offer a wide range of other non-surgical plasticizing procedures: Hyaluronic acid injections, contouring.