- Elimination of unpleasant odors from the mouth;
- Elimination of bleeding;
- Significant reduction of tooth mobility (and thus the risk of tooth loss);
- Pain relief, prevention of periodontal diseases;
- rapid closure and healing of cavities after tooth extractions;
- Restoration of the natural color and correct anatomical shape of the gums
- prevent further spread of periodontal disease;
- Ensuring osseointegration of implants;
- almost complete reduction of the risk of allergies or rejection of the implant;
- Improvement of the patient's quality of life.
- High tolerance
PRP therapy does not introduce foreign proteins or synthetic substances into the patient's body, which can cause an allergic reaction in allergic patients. The only foreign substance that can cause an allergic reaction in a patient is the anticoagulant used to obtain the treatment substrate. Therefore, before prescribing the procedure, it is necessary to determine whether the patient has had a previous allergic reaction to the drug to be used.
- Minimum number of contraindications and possible side effects
The introduction of autoplasm does not cause cell mutations that can cause the growth of benign and malignant tumors. Since the plasma is completely non-toxic, kidney and liver damage, the development of dysbacteriosis and the occurrence of other serious complications from the injection are completely excluded. With proper pre-cleaning of the oral cavity and compliance with the rules of asepsis, the risk of local inflammation is also practically reduced to zero.
Direct contraindications to the administration of autoplasm injections are only bleeding problems and/or bleeding sequelae manifested by a decreased platelet count below 100,000/μl and anemia (hemoglobin below 90 g/l), as well as intolerance to anticoagulants and coagulants.
In addition, caution and a discriminating approach are recommended when prescribing the procedure to patients with coagulation disorders, febrile patients, people with oncopathology, and active herpetic and other viral infections. Relative contraindications include the use of heparin-based medications on the day of PRP administration.
In all other cases, platelet-rich plasma can be administered without restriction.
- Exceptional efficacy
PRP treatment of patients with periodontal disease strengthens gum tissue and prevents the development of periodontitis, which in turn helps prevent tooth loosening and tooth loss.
PRP therapy is very effective in periodontitis treatment
The injections of autoplasm accelerate the healing of implants and prevent their rejection. They also greatly shorten the healing time after extensive maxillofacial surgery, including osteoplasty and sinus inlay.
PRP is essential for dental extractions in diabetics - the injection of platelet-rich plasma ensures rapid wound healing and prevents the formation of abscesses.
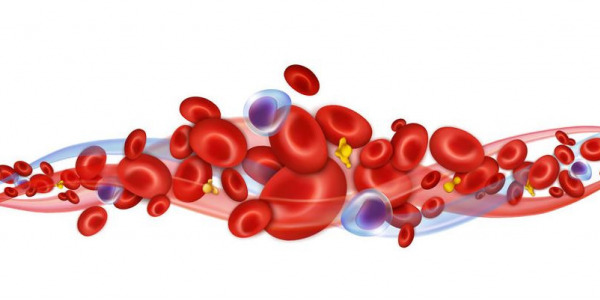
Platelet rich plasma is an autologous plasma volume with a 4-5 fold increase in platelet concentration and is a proven source of growth factors such as PDGF, TGF, IGF, VEGF, EGF, platelet derived angiogenesis factor and platelet factor IV . The positive influence of PRP on bone healing is attributed to the angiogenic, proliferative and differentiating effects of PDGF and TGF in high concentration
The use of PRP technology, in addition to supporting bone healing during extensive bone augmentation procedures, is recommended for all patients with impaired wound healing, such as heavy smokers, diabetics, especially with known wound healing and osteoporotic diseases.

























































































Comments (0)